
Funding Down, Temperatures Up: The Struggle to Protect Women in a Warming World

Across Sierra Leone, it’s ubiquitous small talk—in line at the bank, as people fan themselves at breakfast, and during miles-long walks to get water: “Plac de ot o!”
Translating to “the place is hot,” the Krio language colloquialism encapsulates a harsh truism: that even in a country accustomed to high temperatures, the heat feels increasingly relentless.
Sierra Leone ranks among the world’s most climate-vulnerable nations. Along with heat, Sierra Leoneans live with rising sea levels, coastal erosion, and erratic rainfall.
The changes have outpaced people's ability to identify, name, and address climate change—and its disproportionate impact on women and children, says Leeann Rizk, country director of the Mama–Pikin Foundation, a nonprofit focused on improving the health of Sierra Leone’s women, children, and families. (Mama–pikin means “mother-child” in Krio.)
“Climate change is everywhere, but it’s nowhere. There is no name,” Rizk says. Yet it is deeply felt by pregnant women, dehydrated and fainting from extreme heat while selling goods with children in tow, missing prenatal visits, or forgoing anti-malaria bed nets because the nylon material is too hot to sleep under; and by irritable babies uninterested in breastfeeding.
Just about every aspect of climate change is more hazardous for pregnant women and mothers—especially in low-income countries, says Michele Barry, senior associate dean of Global Health at Stanford University and director of the Stanford Center for Innovation in Global Health. Extreme weather events increase stillbirths, low birth weights, pre-eclampsia, and developmental malformations. Climate disasters disrupt access to contraception, abortion services, and pre- and postnatal care. Women, who are largely responsible for relocating families during climate disasters, make up 80% of climate refugees, according to UN estimates. Heat waves also correlate with increased gender-based violence and homicides.
But resources to adapt to these challenges are scarce: “Women have less access to financial resources for resiliency and recovery, particularly after extreme weather events,” says Barry.
And financing continues to slow. Delegates at last November’s COP30 climate change conference pushed the target date for countries to triple climate adaptation finance from 2030 to 2035—with no clear plan to meet the new deadline. The delay could further stall short-term funding to help low-income countries adapt to climate change’s harshest effects—at a time when adaptation funding should be a top priority, says Barry, who called climate “the biggest health problem now in global health.”
For grassroots organizations focused on climate adaptation, these challenges mean that instead of expanding their reach, they face an existential threat. Mama–Pikin, for example, was just getting started, completing their first mission—to name and explain to Sierra Leonean women how their experience of unbearable heat was connected to other deepening challenges—last year, Rizk says.
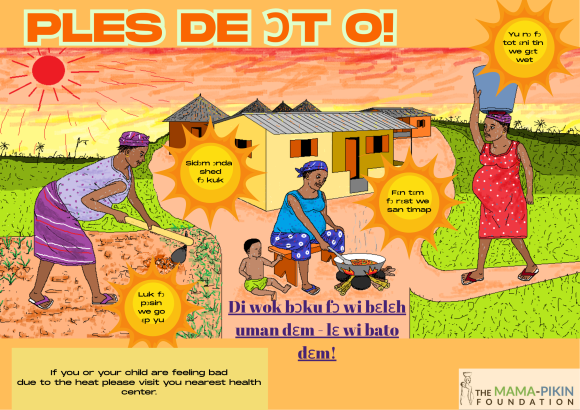
Mama-Pikin launched “Plac de ot o! A Sierra Leone Maternal and Child Health Literacy Tool,” in January 2025. The flip-chart tool uses illustrations depicting everyday Sierra Leonean life to facilitate discussions with pregnant women, lactating mothers, health care workers, and communities. Topics include the challenges of caring for children while pregnant in extreme heat, climate change’s role in a devastating 2017 mudslide that killed over 1,000 people, how developed nations’ pollution ended up on Sierra Leone’s shores and in their air, and more. It also provides practical adaptation strategies using local knowledge, such as creating shade structures with trees, painting tin roofs white to promote cooling, and emphasizing the need for cooling and hydration so that communities can prioritize women’s needs, even when access to clean water is a challenge.
With an initial $30,000 grant from Panorama Global, the program reached approximately 1,972 people from January 2025 through January 2026 through hospital-based learning sessions, professional trainings, community discussions, and other activities.
They made an impact.
After a Princess Christian Maternity Hospital session attended by 144 pregnant women, several said the tool improved their understanding of how extreme heat, flooding, and water shortages could affect pregnancy outcomes, nutrition, and access to care. One woman shared that she had previously attributed frequent dizziness and fatigue solely to pregnancy but now recognizes heat exposure as a contributing factor; she committed to prioritizing hydration, rest, and seeking shade.
“You don’t need rocket science; sometimes it’s just keeping communities informed about weather patterns and helping them understand very simple behavior change messages. But that work has to be done,” says Sono Aibe, an independent consultant to Panorama Global, which provided initial grant funding to the Mama–Pikin Foundation.
Yet within the next few months, Rizk and most of the organization’s staff will be let go, and the organization’s future is uncertain. The team’s next step had been to scale the project, attract national attention, and eventually integrate it into clinic design and rehabilitation plans—and share it with other African countries with similar needs. Now, Rizk says, they won’t be able to do the work.
Grant options to re-up funding—including an expected maternal and child health grant from USAID—have “pretty much dried up,” she says.
It’s especially disappointing because Mama–Pikin has seen how programs can soar—and change health systems—with adequate funding and support, says OB-GYN Fatu Forna, who founded Mama–Pikin 15 years ago with her husband, also an OB-GYN. Six years ago, Sierra Leone—which has one of the highest maternal mortality rates in the world—had fewer than 10 OB-GYNs and less than 10 pediatricians for 8 million people. The Mama–Pikin Foundation partnered with the Ministry of Health to create Sierra Leone’s first OB-GYN and pediatric residency program. It has now graduated its first few cohorts and “has been well integrated into the ministry’s work, which was the plan all along—to make it sustainable,” says Forna.
But for small NGOs working on perhaps the most neglected corner of the climate response—climate adaptation for sexual and reproductive health—sustainability has been unattainable, Forna says. Larger organizations “will probably survive and cut down their impact, but for small local organizations, they just cease to exist,” she says.
Women’s sexual and reproductive health is already chronically underfunded even without climate stressors, says Barry. Less than 0.5% of climate health financing reaches health initiatives, and of that tiny fraction, even less reaches women’s health programs.
And of the funding that is available, mitigation efforts—such as reducing emissions—typically account for over 60% of total climate financing efforts, while adaptation receives roughly 25%–30%. In 2022, that amounted to over $1 trillion globally for mitigation, and $68 billion for adaptation.
Meanwhile, countries forced to adapt to climate change are doing so at great cost to their health, and their bottom line.
In Uganda, for example, climate-related disruptions to sexual and reproductive health services in two districts are costing the health system an estimated $20 million per year, according to an analysis conducted by Pathfinder International. That includes over $7 million in preventable health care costs (every $1 not spent on contraception costs $3.77 in maternal care), 64 avoidable maternal deaths, and 614 preventable newborn deaths. Scaled nationally, those costs would exceed $950 million per year.
Plus, most climate financing comes as loans rather than grants—and paying them back often means raising taxes, says Tabinda Sarosh, CEO of Pathfinder International. For loan decisions, adaptation efforts take a back seat to infrastructure projects or other health needs, “which of course require due attention—but that does not mean that mothers’ health, children’s health, girls’ health, and their reproductive health should get deprioritized.”
In the current funding environment, climate action groups are working to do their own kind of adaptation, by diversifying their funding sources.
Even after achieving record funding in 2025, the Green Climate Fund—the world’s largest dedicated fund helping developing countries reduce greenhouse gas emissions and adapt to climate change—is seeking new ways to shore up funding by exploring capital markets and concessional loans. The group, funded mostly by voluntary contributions from wealthier countries, aims for an even split between adaptation and mitigation efforts.
Engaging the private sector can pay dividends, especially for the most complex adaptation projects. For example, Pathfinder received a $10 million grant from Takeda Pharmaceuticals to implement a four-year program to help maintain access to sexual and reproductive health services during emergencies and climate crises. The initiative included training health providers on the Minimum Initial Service Package (MISP) for Sexual and Reproductive Health, a set of lifesaving, priority, and coordinated activities implemented at the onset of a humanitarian emergency to prevent mortality and morbidity among crisis-affected populations; supporting facility renovations; and facilitating disaster management committee meetings. After the project, overall emergency preparedness scores in Bangladesh jumped from 39% to 54%; and in Pakistan, from 54% to 72%.

Poonam, a climate advocate in Sindh, Pakistan, worked with Pathfinder International to help families protect themselves from vector-borne diseases and ensure pregnant women prepare for climate emergencies. August 2025. Photo Courtesy of Pathfinder International
“Targeted interventions work,” says Sarosh—and ideally come in the form of long-term investments. Historically, climate adaptation has faced a Catch-22: Inadequate funding to disseminate adaptation efforts has made it difficult to provide evidence of their value. But that is no longer the case, she says: “We have enough evidence. Now let’s move into action.”
Committing to a new era of sustainable financing for climate change means acknowledging that while mitigation is crucial, the need to adapt is already here.
Many who make decisions about climate financing—mostly men in wealthy countries yet to experience firsthand the worst impacts of climate change—“are still dreaming that some miraculous tech is going to save us. But for developing countries, [the impacts are] happening now,” says Aibe.
Join the 50,000+ subscribers in 170+ countries who rely on Global Health NOW summaries and exclusive articles for the latest public health news. Sign up for our free weekday newsletter, and please share the link with friends and colleagues.
Pregnant women attend a demonstration of the “Plac de ot o!” climate literacy tool at Princess Christian Maternity Hospital in Freetown, Sierra Leone. May 2025. Photo Courtesy of the Mama–Pikin Foundation


